How does the SARS-CoV-2 virus really spread? Presenting a theory that might explain the super-spreader

Mail This Article
The exact mechanism of spread of the SARS-CoV-2 virus in the community has so far been unclear. Droplet spread by coughing and sneezing has been the conventional explanation. However, recent observations have suggested this might not be the only mechanism, as people without any symptoms have even become super-spreaders. Based on published research evidence, this article proposes the role of aerosols, but in a manner that has not been discussed before.
It is well-known that aerosols loaded with virus are generated in the ICU during procedures such as intubation on a patient with COVID-19. Perhaps unknown to many is the fact that the human body also routinely generates its own aerosol - through the use of vocal cords. Researchers have shown that even everyday conversation generates aerosols, as air squeezes past the already moist vocal cords. Also termed the 'fluid film burst' theory, this is somewhat like pressing the button of a deodorant spray.
The SARS-CoV-2 virus is present in large numbers in the throat of a person before the onset of symptoms. Even though such people do not cough or sneeze, they are well-known to spread the virus, sometimes even as super-spreaders.
There is evidence that when a person talks in a closed space, the throat secretions get aerosolised. This is an efficient way to spread the virus to the next person. The longer the time spent sharing the closed space, the greater the dose of virus inhaled by others. The Washington choir example with an unprecedented attack rate of 75% stands as the strongest evidence for this theory playing a major role in the spread of SARS-CoV-2 by apparently healthy people. This theory unifies numerous other observations of superspreading events that have so far defied explanation.
It is therefore proposed that aerosol generated through everyday conversation by asymptomatic people is one the main routes of spread of the SARS-CoV-2 virus, especially in closed gatherings. Once validated, this will have significant impact on the nature of control measures taken hereafter.
The way ahead
One of the most important challenges faced by mankind at this time is to find a way to arrest the spread of the SARS-CoV-2 virus. The purpose of this article is to interpret recent observations in the light of published scientific research, to get a better understanding of the way forward. As the SARS-CoV-2 that caused COVID-19 is still a new virus, there is greater need to observe keenly, remain open-minded and strive for evidence-based solutions.
Why do some people become super spreaders? What is the fluid-film burst theory?
Throughout history of epidemics, there are documented accounts of 'Poison Kings' or people who spread the disease to disproportionately large numbers of people (See ref. 28 below). A man admitted to a Hong Kong hospital is documented to have infected 138 people with SARS-CoV-1 virus (Ref. 9). The episode in the Washington state church choir where 45 out of 60 seemingly healthy people got infected within three weeks is a well-documented example of the super-spreading potential of the SARS-CoV-2 virus (Ref. 20). The attack rate in that case was 75%, substantially higher than previously thought.
The obvious question was whether an individual who attended the choir sent out large numbers of tiny droplets containing virus into the air, that got inhaled by the people around over a period of two and half hours that they spent in the closed space together.
A study published in Nature a year ago has the answer to this question (Ref. 8). A group of volunteers were asked to speak in varying loudness, while their droplet emission was measured. The findings were:
1. Speaking louder produced up to ten times more droplets
2. Some people emitted more droplets than others for the same loudness
3. Each individual had a unique and consistent pattern of droplet production
4. The mean droplet size was I µ (about 1/75 the thickness of hair), and remained unchanged regardless of the loudness of speech. These are smaller and lighter than the 50 µ droplets produced by coughing and sneezing. They could potentially be more infective as they stay in the air longer, spread wider and get inhaled deeper.
5. Among breathing patterns, deep exhalation produced more droplets (Ref. 10)
Many people assume that vocal cords are only involved with production of voice and with coughing. Hence it is important to understand the process of speech in greater depth.

While speaking, the cords first come together. Along with this, a thin film of fluid forms between the cords. Next, air gets pushed out of the lungs through the nearly closed cords. As the cords vibrate, voice is generated (Ref. 26). The fluid that coats the cords consists of throat secretions containing large numbers of viruses. This fluid film gets nebulised almost like when we push down on the button of a deodorant spray. The harder the button gets pressed, the more droplets get released. The authors put this forward the as 'fluid film burst' theory (Ref. 8).
Applying the results of this study to the Washington choir example, the super-spreader was able to generate sufficient droplets to infect 75% of the people in that room.
Anyone who has blown bubbles will relate to the fluid film burst theory. If air is blown too hard through the soap film, instead of producing a bubble, the film bursts and tiny droplets get spurted all over one's face.
What is the difference between droplet, aerosol and airborne transmission?
These are commonly heard terms and can be confused for one another.
Droplets are blobs of mucus that get ejected into air as a result of a cough or a sneeze. They settle down quickly due to gravity as they are relatively bulky and heavy. Their size is about 50 µ (Ref. 8). They are commonly spread within a six feet distance around the subject. They can be figuratively compared to throwing water-filled balloons.
Aerosols are made of really small droplets. They are less than 5 µ size, and can be figuratively compared to cigarette smoke or mist. They are too light to settle immediately by gravity, and float in the air for a longer time than large droplets. They also travel farther than droplets, and can get blown about a closed room by air currents. This occurs when the velocity of the circulating air exceeds the natural descending velocity of the droplet (Ref. 12), and happens in enclosed buildings.
In hospitals, aerosols get generated while procedures like tracheal suction, intubation and ventilation are performed on patients. Studies have shown SARS-CoV-2 virus can remain viable in aerosols for about three hours (Ref. 16). They may deposit on surfaces and make them infective.
There is mild difference of opinion about the exact size cut-off between large droplet and aerosol. However, particles generated by normal speaking are only 1 µ in diameter (Ref. 8), and can easily be classified as aerosol.
Airborne transmission occurs in diseases like measles, influenza, chicken pox and tuberculosis when viral and bacterial particles getting suspended in air, travelling long distances in the wind. The smaller the size of the particle, the longer it stays in the air. It is not known yet whether SARS-CoV-2 virus is an airborne pathogen.
Various modes of respiratory virus transmission have been described in detail by Kutter et al (Ref. 12).
Could the aerosol theory explain Italy's predicament? How does lockdown compare between India and Italy?
The role of aerosol in spreading the SARS-CoV-2 virus when crowds gather in closed spaces is increasingly apparent. An early example was reported from the city of Daegu in South Korea, where over 85% of the initial COVID-19 cases were tracked down to the Shincheonji church (Ref. 30). Numerous similar super-spreading events have been reported from all over the world (Ref. 31-34)
The rapid spread of COVID-19 in Italy could potentially be explained by the fact that one out of five of the 60 million people in that country go to church gatherings at least once a week, the highest attendance in western Europe (Ref. 19). The majority of those who attend church in Italy are elderly people (Ref. 29). Numerous super-spreading events through aerosols could have occurred, as was the case with the Washington church choir (Ref. 20). By the time partial lockdown was announced on March 12, the virus could potentially have reached many households.
Public gatherings were partially stopped in Italy only six weeks after the first case was reported in the country, and three weeks after spread was detected. By then, 15,113 people were already diagnosed with the infection, and 1016 people had died. Full lockdown occurred 10 days later on March 22. By then, 59,138 people were infected, and 5476 people had lost their lives.
While fighting a pandemic like COVID-19, it is important to learn from other nations, and estimate the impact of these measures in a local context. To convert the above timeline into the Indian scenario, a few basic calculations may be made. India's population being 20 times that of Italy, applying a factor of 20, these measures are approximately equivalent to locking down the country after 12,00,000 people got infected and 100,000 died.
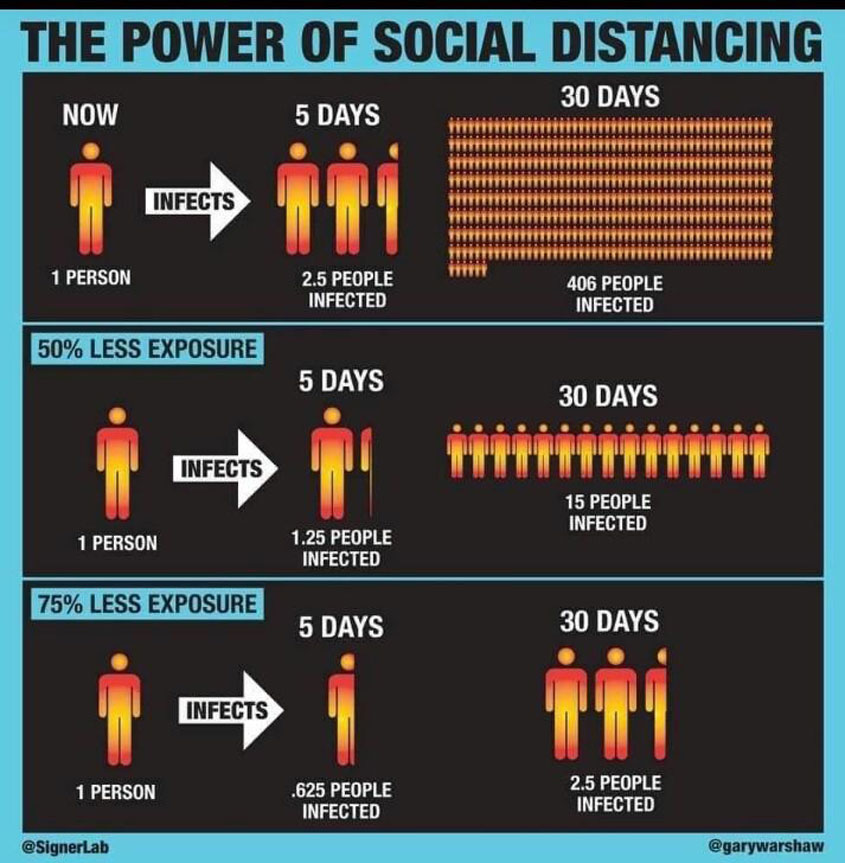
In contrast to Italy, India's lockdown measures were initiated relatively early on March 22, at a time when the total number of cases was only 396, and only 10 deaths had occurred. The measure was announced on national television by the prime minister within 17 days of the first reported spread in India and enforced within 22 days, in contrast to 31 days taken by Italy. A full lockdown has been in effect in India since March 24. It is known that when it comes to lockdowns, timing is crucial. Even a three-week delay of initiating lockdown is estimated to result in an 18-fold rise in the number of cases and deaths (Ref. 22, 23).
It must however be noted that the low testing rates in India and the higher density of the population would limit a direct comparison.
Does air-conditioning cause spread of COVID-19?
This is a question that has been asked by many, but for which clear answers are not yet available. A widely quoted paper from China reports that the SARS-CoV-2 virus spread among three families that happened to dine at an air-conditioned restaurant (Ref. 11). The authors hypothesise that droplets from the index patient got blown at the neighbouring tables by the air-conditioner as shown in fig 2.
Rather than the effect of air-conditioning, the lack on natural ventilation and the fluid-film burst theory appear more likely to explain what happened at this restaurant. The families shared the same space, their visit overlapping by well over an hour. The conversation must have generated an aerosol that travelled to the nearby tables.
The closed nature of the space and the proximity of the tables must have played a role. However, swabs taken from the air inlet and outlet were negative. None among the restaurant staff got the virus, which means that there was no airborne transmission, and all spread occurred through tiny droplets.
The problem with business meetings in closed spaces
The aerosol theory holds true for other common scenarios, such as business meetings where several people speak and spend time together within a closed space. The following is a published report of how COVID-19 spread from China to Germany (Ref. 2).
This is the timeline of patient 1 in Germany getting the virus from a visitor from China, and then spreading the virus to patient 3 and 4 who were colleagues. No one who attended the meeting had a cough or sneeze. What is remarkable here is that the Chinese woman (index patient) developed symptoms only after she left Germany (Ref. 2)
The symptoms of patient 1 and 2 started within three days of attending meetings with the Chinese woman, and disappeared within three days. This timeline highlights the quick spread of the virus between people, as well as the short duration of symptoms in mild cases.
This incident is also consistent with the theory of aerosol spread, a natural outcome when people speak at meetings held in closed rooms without natural ventilation. Traditional healthcare models where patients converge from multiple geographic locations and have conversations with doctors and nurses within closed spaces is another area of concern. Air samples obtained from high traffic areas within hospitals have already shown the presence of the virus (Ref. 15).
It is clear from the above discussion that the traditional six feet social distancing and handwashing will not be enough to limit the spread of COVID-19. Strategies that specifically target the aerosol spread by asymptomatic patients in closed spaces might hold the key to defeating the virus.
The unknown number of asymptomatic people who are spreading the virus in the general population, coupled with the limited ability of several countries to test for the virus poses a challenge. As Dr Tedros Adhanom, director general of the WHO said, "You can't fight a virus if you don't know where it is." Given the numerous recent instances of super-spreading events, group gatherings are to be avoided until the pandemic is brought fully under control, as flare-ups are possible otherwise.
(The author is a senior consultant gastroenterologist and deputy medical director, Sunrise Group of Hospitals).
Further reading:
2. Visitor from China gives virus to Germans at a business meeting
3. The first patient who had COVID19 in the US, reported travel to Wuhan. He was isolated promptly and did not infect any others, including the caregivers. He developed breathing difficulty on Day 5 of admission, progressing into what seemed to be bilateral patchy pneumonia, but improved by Day 8. Click to read
4. Report of the first 18 patients in Singapore
5. The first major hospital outbreak of COVID-19 in India, at Mumbai occurred basically because it is impossible to predict who has COVID-19 or not. It is safer to assume everyone has it, and take standard precautions. Click to read
6. Large gatherings and communicable diseases: a review
10. How aerosol particle size varies with breathing pattern. Deep exhalation produced more droplets.
11. Virus spread among neighbouring tables at a restaurant in China
12. Modes of transmission of respiratory viruses
13. The science of droplets and airborne transmission of germs
14. Study of the environment of three COVID-19 patients admitted to isolation rooms in Singapore. Extensive environmental contamination occurred in one patient. Air vents of the room were positive for the virus for one patient, indicating extensive droplet spread. However, air samples were negative for virus. Click to read
15. Virus-containing aerosols were detected in crowded public areas in hospital settings. The authors raise the possibility of aerosols being generated after droplets settles on surfaces, including PPE worn by healthcare staff. Click to read
16. COVID-19 can remain viable in aerosol for three hours, widely quoted study published in NEJM
18. One out of five Italians attend church at least once a week
19. Italy locks down on March 22
20. Super-spreader event was documented at a church choir in Skagit County in Washington state, US. Among 60 people who showed up for the choir, 75% got sick within three weeks, including two deaths. They had spent 2 ½ hours at the church, with standard precautions reportedly avoiding all physical contact. The attack rate of 75% is remarkably higher than previously thought. This raises the possibility of droplet or aerosol spread in a closed room among well-looking people, as a result of forceful respiratory manoeuvres. Click to read
21. Droplets travel farther than we thought: new evidence published in JAMA March 26
22. Timing of social distancing saves lives
23. Evidence based answers to 25 Questions that doctors ask about COVID-19: Dr Rajeev Jayadevan
25. Protecting healthcare workers - an evidence-based approach, Dr Rajeev Jayadevan
26. Aerosol and droplets: Classifications vary
27. Video of vocal cords vibrating while singing shows the potential of aerosol generation
28. Poison King is the term used to describe a super spreader
29. The majority of those who attend church in Italy are over age 65
30. South Korean church becomes the epicentre of a large outbreak
31. Buddhist temple accounts for 10% of the initial COVID19 cases in Hong Kong
34. Nearly a third of India's known COVID-19 cases are linked to the religious gathering at the Markaz